Case 1: AML with mutated NPM1
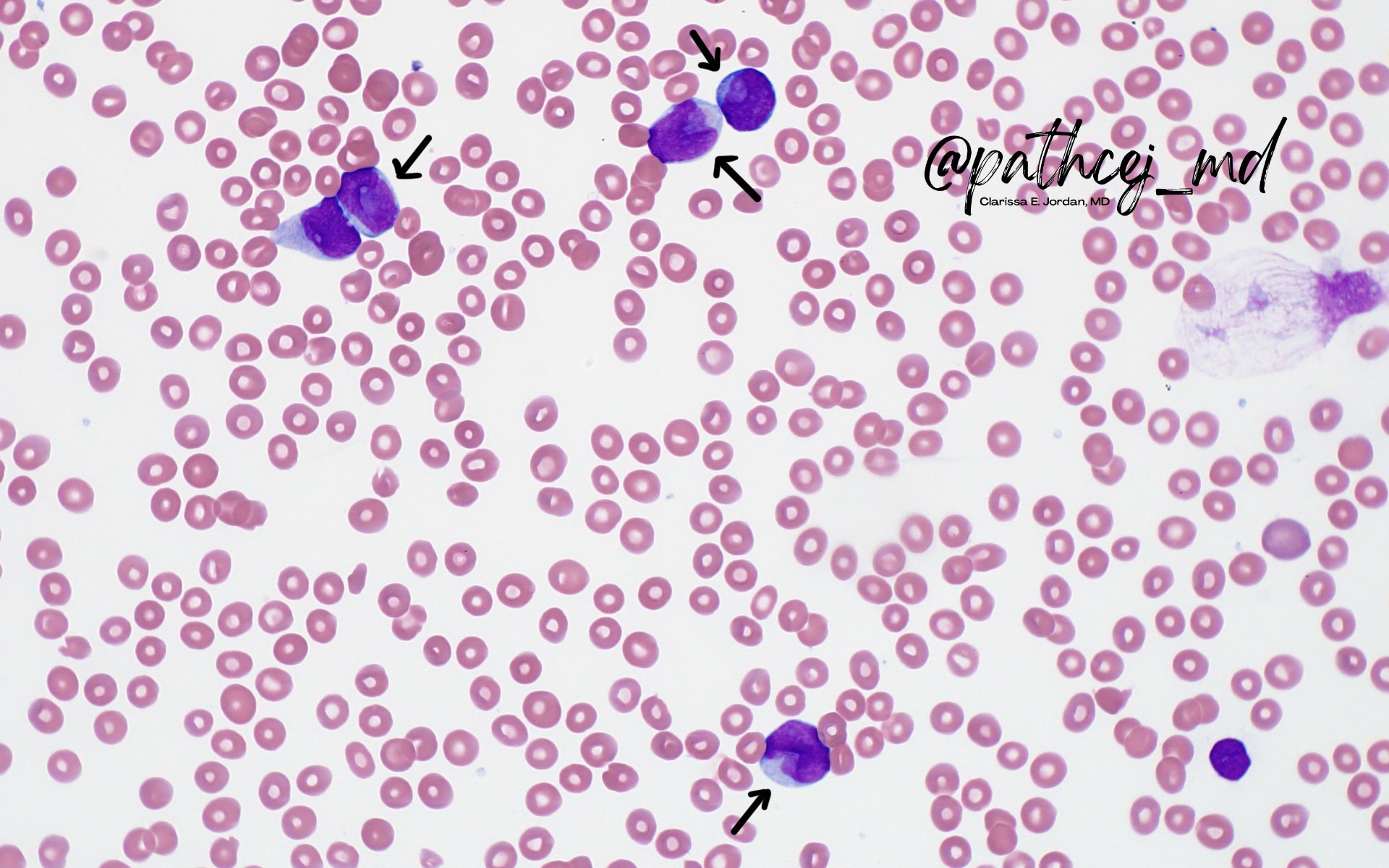
Blasts with this morphology are highly-associated with NPM1 mutations (particularly when there is a coexisting FLT3-ITD)
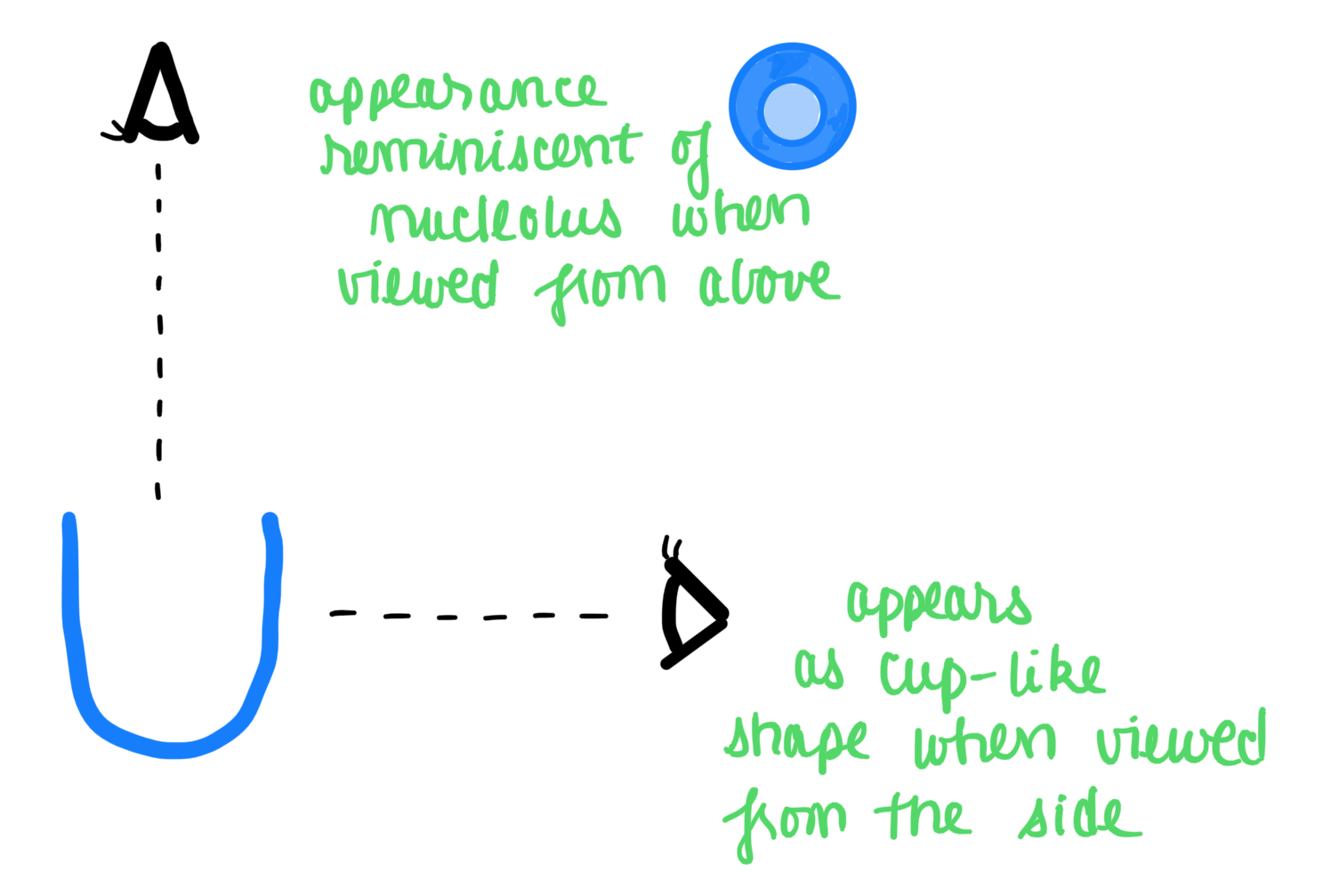
Note that the blasts are medium-sized, with high N:C ratio, and many have an indented nucleus, leading to a cup-like shape
This is especially apparent when viewed in profile, and can resemble a nucleolus when viewed head-on
On ultrastructural examination, these indentations are filled with mitochondria, lysosomes, and endoplasmic reticulum
🔎 AML with mutated NPM1 (4 bp insertion into exon 12) occurs in 25-35% of of adult AML. Generally associated with favorable prognosis, but is a clinically heterogenous group, as it is usually associated with other mutations (e.g. FLT3-ITD)
⚠️ Pitfalls:
- Features of AML w monocytic differentiation (like nuclear clefts and folding) can be reminiscent of cup-like nuclei
- Cup-like nuclei can resemble cleaved nuclei in APL, (esp since AML w mutated NPM1 often shows CD34➖and HLA-DR➖), but PML-RARA would be ➖
Thanks for following along! 🤗
Special thanks to Dr. Dan Larson for his excellent teaching on this case!
Find this case on Twitter:
🩸#Hematopathology case #tweetorial 🧵:
— Clarissa E. Jordan, MD (@pathcejmd) December 17, 2021
If you you had to guess, a mutation in which of the following is most likely in this case of AML? (Poll ⬇️) #HemePath #PathTwitter #path2path (new to tweetorials, so I welcome any feedback!) @MayoClinicPath @KMirza @AaronGoodman33 pic.twitter.com/6T1uQtYx3t